Here is some in depth feedback from “Guest Blogger” Dr. Emmanual Favaloro on the subject of lupus anticoagulant chronicity raised by Pam Owens of TriCore Laboratories, Inc in a Feb 29 post. I sent the highlighted questions to Dr. F on Feb 27:
When an LA/APA is defined as “chronic,” does it wax and wane?
Not normally according to my understanding, but you have to take into consideration the lab doing the test(s) and the individual patient circumstances. In regards to lab testing, there are both false positive and false negative LA/APA test results. Patients may alternatively have transient LA/APA related to infection (etc). Patients with true LA/APA may get better and then have relapses. So, with most cases of true LA/APA, persistence and repeatability of testing can be shown. But sometimes this isn’t the case. A good paper to check is: Erkan D, Derksen WJ, Kaplan V, Sammaritano L, Pierangeli SS, Roubey R, Lockshin MD. Real world experience with antiphospholipid antibody tests: how stable are results over time? Ann Rheum Dis. 2005 Sep;64:1321-5.
Or does intermittent positivity more likely signal transient innocent responses to drugs or inflammation?
See above response. It is important to retest in ~12 weeks to confirm the initial finding and check persistence. No point testing once and then rechecking every few years – how do you know the first result was a real/persistent LA/APA; could have been a false positive.
How did Dr. Pengo’s committee come up with the 12 weeks interval?
I’m pretty sure Pengo’s committee just ‘copied’ this 12 week period from the APA guidelines (Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2006; 4: 295–306.). The original guidelines (Wilson WA, Gharavi AE, Koike T, et al. International consensus statement on preliminary classification criteria for definite antiphospholipid syndrome. Arthr Rheum 1999;42:1309-11.) said 6 weeks, but I believe that some experts on the revision committee had experience with some ‘transient’ LA/APA that ‘persisted’ for longer than 6 weeks, so they moved this interval to 12 weeks. I don’t think there’s a lot of scientific evidence around the specific value of ’12 weeks,’ but this should be long enough to exclude ‘transient’ LA/APA due to drugs/infection/etc.
Finally, from our EQA experience, we know that samples can be collected from patients with LA/APA every year or so (with their permission of course) for EQA challenges, and sometimes their levels change and at other times they are quite ‘stable’; however, although the medians from returned data are similar between collections, the (inter-lab) ranges are always wide – and importantly are reported as negative in some labs but positive in others. I have attached a figure from one of my pending papers. The legend is as follows:
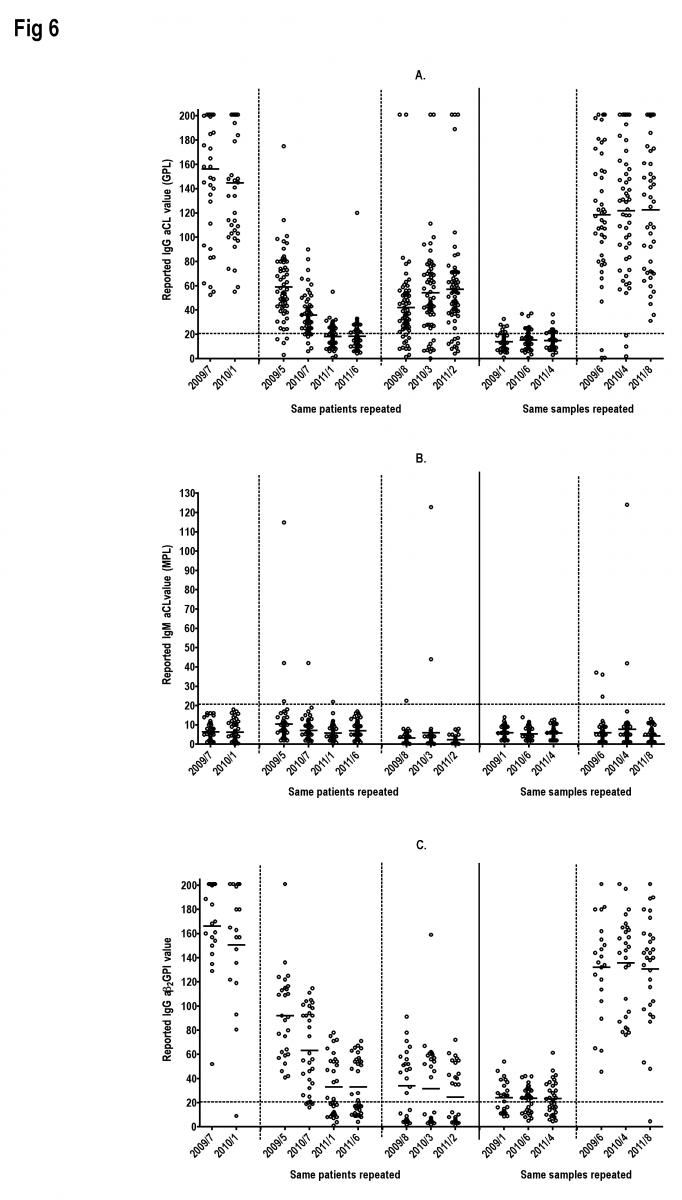 Results of repeated testing of the same patients (but different collections; left portion of figures) or of the same samples (viz, same patient collections; right portion of figures) in different EQA test challenges. The same patients/different collections vs same patient collections are separated by the unbroken vertical line, and each separate repeat patient is separated by the dashed vertical lines. The same patient collections tested at different times (right portion of figures) yielded similar medians and ranges. The same patient/different collections tested at different times sometimes yielded similar medians and ranges (highlighting a stable aPL) and sometimes showed discrepant medians and ranges (highlighting a less stable aPL, or fall in titre over chronological time, which may be treatment related).
Results of repeated testing of the same patients (but different collections; left portion of figures) or of the same samples (viz, same patient collections; right portion of figures) in different EQA test challenges. The same patients/different collections vs same patient collections are separated by the unbroken vertical line, and each separate repeat patient is separated by the dashed vertical lines. The same patient collections tested at different times (right portion of figures) yielded similar medians and ranges. The same patient/different collections tested at different times sometimes yielded similar medians and ranges (highlighting a stable aPL) and sometimes showed discrepant medians and ranges (highlighting a less stable aPL, or fall in titre over chronological time, which may be treatment related).
so, as I said; you have to be wary about repeatability of LA/APA; when patients are sometimes positive and sometimes negative, is this from testing in the same laboratory, and is it a good laboratory?
cheers, Emmanuel

Thanks George and Dr Favolaro! We would like to think we are
Thanks George and Dr Favolaro! We would like to think we are a good lab and are only looking at the results we have previously generated. Our biggest bug is preanalytical. Being a reference lab, we do not get the luxury of processing all our specimens and always have this in mind when looking at inconsistent results.
Pam