From Eleonor Arellano: Thank you for presenting a very informative seminar, “Whatever Happened to the PT and PTT?” about the new anticoagulants last Friday at Rancho Mirage. Our ER physician is requesting the laboratory to increase the reporting of international normalized ratio (INR) of ER patients up to 10.0 INR. What are your thoughts about that? Why do you think it is necessary for ER patients? Any significance that you know of?
Hello, Eleonor, and thank you for your question. 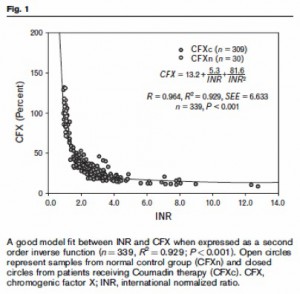 This figure is published in McGlasson DL, Romick BG, Rubal BJ. Comparison of a chromogenic factor X assay with INR for monitoring oral anticoagulation therapy. Blood Coag Fibrinolys 2008;19:513–17. The article describes how the clot-based and the chromogenic factor X assays relate to the INR and this figure illustrates the relationship of chromogenic factor X results with the INR in normals and people on Coumadin whose results are either within or above the therapeutic range. The portion of the curve that is above INR 4.0 is nearly flat, illustrating how little change there is in factor X levels in relation to INR when the INR is over 4.0. In fact, as I mentioned in my presentation last week, any INR over 4.0 (a minority of labs prefer 5.0) requires an immediate contact with the physician, pharmacist, or nurse who is managing the patient. Whether the INR is 5 or 10 shouldn’t change the lab’s call-back requirement nor the physician’s approach to managing the patient in the ER. What is important, of course, is for the physician to treat for INR in the presence of bleeding. The full guidelines for management of bleeding in Coumadin overdose are published in Ageno W, Gallus AS, Wittkowsky A, et al. Oral anticoagulant therapy: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (9th edition). Chest 2012;141: e44S–e88S. Your physicians probably have access to this publication. I hope this helps.
This figure is published in McGlasson DL, Romick BG, Rubal BJ. Comparison of a chromogenic factor X assay with INR for monitoring oral anticoagulation therapy. Blood Coag Fibrinolys 2008;19:513–17. The article describes how the clot-based and the chromogenic factor X assays relate to the INR and this figure illustrates the relationship of chromogenic factor X results with the INR in normals and people on Coumadin whose results are either within or above the therapeutic range. The portion of the curve that is above INR 4.0 is nearly flat, illustrating how little change there is in factor X levels in relation to INR when the INR is over 4.0. In fact, as I mentioned in my presentation last week, any INR over 4.0 (a minority of labs prefer 5.0) requires an immediate contact with the physician, pharmacist, or nurse who is managing the patient. Whether the INR is 5 or 10 shouldn’t change the lab’s call-back requirement nor the physician’s approach to managing the patient in the ER. What is important, of course, is for the physician to treat for INR in the presence of bleeding. The full guidelines for management of bleeding in Coumadin overdose are published in Ageno W, Gallus AS, Wittkowsky A, et al. Oral anticoagulant therapy: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (9th edition). Chest 2012;141: e44S–e88S. Your physicians probably have access to this publication. I hope this helps.

How an INR within 510 might affect physician decision is p
How an INR within 510 might affect physician decision is presented in a recent British guideline:
Recommendation: Patients with an INR greater than 5.0 but who are not bleeding should have 12 doses of warfarin withheld and their maintenance dose should be reduced (1B). Patients with an INR greater than 8.0 should receive 15 mg of oral vitamin K (1B).
Guidelines on oral anticoagulation with warfarin–fourth edition, 2011
http://www.bcshguidelines.com/documents/warfarin_4th_ed.pdf
Some publication suggest that initial INR within 5-10 might
Some publication suggest that initial INR within 5-10 might be indicative if patients would be undercorrected or overcorrected after warfarin reversal:
According to our protocol, 2 mg of oral vitamin K in addition to omitting the day’s dose of warfarin, were administered to all patients presenting INR levels >or=5.0 and below 10.0; the INR values were checked 20 h after vitamin K administration. The rate of decay of INR, bleeding and thromboembolic complications at presentation and the following 30 days, as well as resistance to warfarin were assessed.
RESULTS: Of the 1,611 events, 1,043 (878 patients) met the selection criteria. The median (interquartile range) INR was 6.64 (6.12-7.52) at presentation (day zero) and fell to a median (interquartile range) INR of 2.72 (2.18-3.52, P < 0.0001) after the vitamin K administration (day one) and 90.6% of the INRs were below 4.5. In 98 (9.4%) instances the INR values did not fall below the safe limit of 4.5 and in 173 (17%) instances the INR values were overcorrected to below 2.0. Median INR value on day zero in these two groups was higher (7.3 vs. 6.6, P < 0.0001) and lower (6.5 vs. 6.7, P = 0.049) than that of the remaining cases, respectively.
—
from Denas G, et al. Effectiveness and safety of a management protocol to correct over-anticoagulation with oral vitamin K: a retrospective study of 1,043 cases.J Thromb Thrombolysis. 2009 Apr;27(3):340-7.
While the recent version of ACCP recommendations for VKA rev
While the recent version of ACCP recommendations for VKA reversal does not contain a detailed guideline, previously published guides (i.e. from AHA/ACC 2003)provide a recommendation for physicians on how to reverse warfarin therapy based on initial INR: “When the INR is above the therapeutic range but below 9 and clinically significant bleeding has not occurred…”
from http://circ.ahajournals.org/content/107/12/1692.full